

Intro Series No.2: How to Coproduce
Oct 02, 2019
Let's #CoproduceCare - Democratising the care debate & uncovering the hidden opportunities for people-led coproduced care.
This series of blogs will explain what coproduction is, what Coproduce Care plans to do and to explore good examples of coproduction. This second blog will explore coproduction practically and talk through some examples of coproduction in action.
Blog 1 Recap: Coproduction by No Other Name
In the first blog we discussed what coproduction is as a concept and its potential to revolutionise how care is provided as a service to actively involve those affected by care or caring. This blog will include a quick recap and then consider examples of those trying to working coproductively in different sectors – don’t forget to tell us of examples in your area so we can share the knowledge and create a coproduction catalogue.
What is Coproduction (figuratively speaking)?
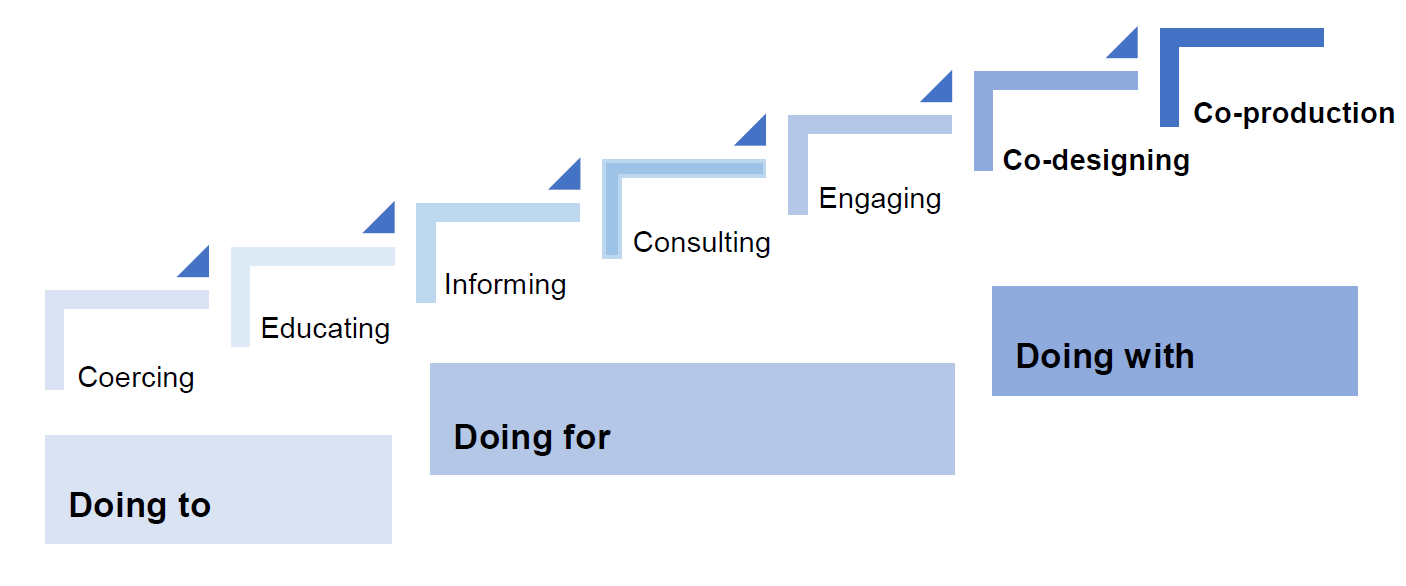
In their recent report, Skills for Care
set out a pictorial version of NEF’s coproduction ladder:
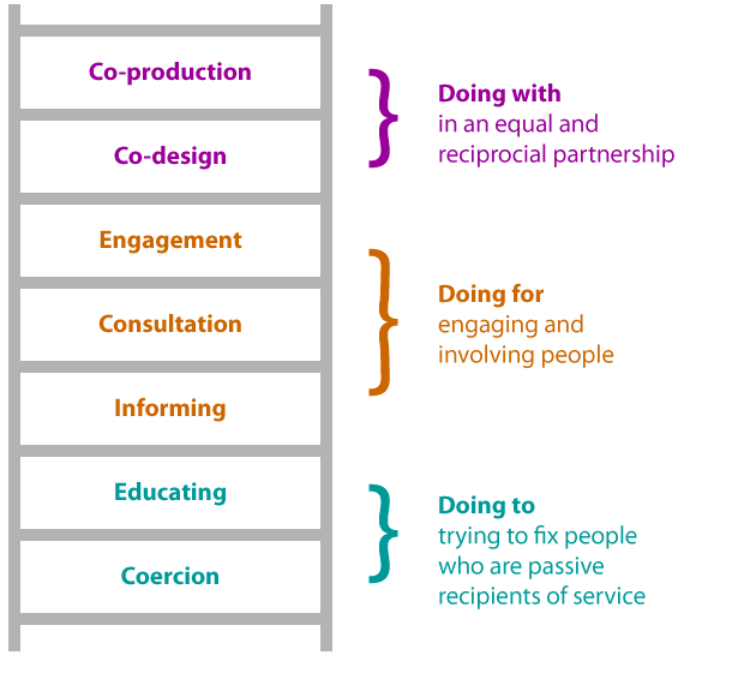
An even more accessible version of the coproduction ladder has been developed byTLAP:
Watch out for the bureaucrats!
There is no legal definition of care, yet the provision of care seems to be increasingly legalistic and bureaucratic. Whilst we have come a long way from Edward VI’s Poor Laws of 1540s which kick started the legitimacy of institutionalised care, a lot of today’s care and caring is focused on policies, procedures, strategies, KPIs, measures, incentives, targets, systems and structures rather than people.
Even across the pond people are coming to the realisation that data entry in health care is becoming mind-numbing and voluminous, resulting in many health care workers suffering from burnout. It can also lead to the individual and their community being lost in the care debate. However, there are some changes afoot. For example, it is promising that social care commissioning now requires organisations to evidence their commitment to Social Value
before being awarded a contract with a commissioning body for health and social care.
Also, the newly created Primary Care Networks
(PCNs), which are set to revolutionise the way GP surgeries operate, are touted as a move towards making health and care more community focused. But even these are poorly understood and fundamentally being developed behind closed doors with professionals rather than people and lacking consultation and therefore coproduced. However, all is not lost. Next, we explore examples of coproduction.
Coproduction Examples
There is some great work being done on coproduction. Previously purely top down organisations are starting to reflect and reform to produce some praiseworthy coproductive moves. These include Manchester City Council , Care Quality Commission and various local authorities which are developing coproduction advocates.
There is some great work being done on coproduction. Previously purely top down organisations are starting to reflect and reform to produce some praiseworthy coproductive moves. These include Manchester City Council, Care Quality Commission
and various local authorities which are developing coproduction advocates.
Manchester City Council
A grassroots movement has been started by Manchester’s Homeless Partnership (MHP). Manchester developed coproductive ways of working leading to better outcomes, recovery and experiences for homeless people. Following a City Conversation, a values-led charter was created. The partnership divided stakeholders into groups. People with experience of homelessness were represented in the groups at all levels, including as chairs of the Partnership Board. The group drove the change, safeguarded agreed values and supported joint working with homeless people and management.
The scheme created a Business Support Group to enable joint decision making in developing the homelessness solution. People with experience of homelessness helped codesign the Big Change MCR
– an alternative giving scheme supporting individuals who are homeless by paying for items they need such as a deposit for a home, a training course, clothes for a job interview, furnishing for a new flat, or travel costs. Their digital platform ‘Street Support’ also links people affected by homelessness with those able to provide support. The Booth Centre for homeless support has contributed to a coproduction toolkit
from its experiences of working with the MHP. Communicating their work to the wider public was a key.
The beginnings of Coproduction in care – Making It Real initiative by TLAP
There are some promising moves towards coproduction both at an organisational and personal level in care. The Making It Real toolkit
developed by TLAP (Think Local Act Personal – a promoter of coproduction in social care) was re-launched last year. The relaunch was born out of Quality Matters, an initiative that is led by the Department of Health and Social Care (DHSC) and has previously been pioneered by the health and social care regulator, the Care quality Commission (CQC) to collaboratively improve the quality of care. Making It Real is exactly what it says on the tin.
TLAP developed the document coproductively with people who use care services and organisations providing services, to create a selection of ‘I’ statements (what people using care services of what they expect from services) and ‘We’ statements (commitments service providers can make to meet people’s needs) to make good quality, inclusive services a reality for people using them. In a sense, it can be used as a care quality benchmark.
‘I’ statements include: ‘Living the life I want, keeping safe and well’, ‘Keeping family, friends and connections’ and ‘Staying in Control’. Whilst the ‘We’ statements of what organisation’s commit themselves to in order to improve the quality of care include ‘We don’t make assumptions about what people can or cannot do and don’t limit or restrict people’s options’ and proactive intentions such as ‘We work with people as equal partners’.
The Making It Real initial has a real potential as a quality assurance for organisation in care to ensure they are operating in a coproductive way and to standardise a system of coproduced care. check out their full document here
and helpful directory TLAP have created
on how organisation are committing to and using Making It Real.
"For example, Hobbs Field care service for adults with a learning disability, has used Making It Real to coproduce their recruitment process. Rather than asking people to attend an interview panel, the home co-designed how people wanted to be involved in recruitment. This resulted in a more informal process. Using pictures, Makaton and signing, people living at the home decided to show candidates around the home and have an informal ‘get to know you’ chat. This resulted in benefits all round. People living in the home felt a sense of pride and in more control of the process. Staff had a renewed sense of codecision-making and the interview candidate was able to express her own values with people living at the home. Coproduction doesn’t have to look corporate or ground-breaking. Sometimes the simplest solutions can be the most effective."
Local Coproduction motions in social care
Many progressive health and social care teams are developing their own coproduction networks.
A useful example is the Scottish co-production network
which shares learning and has an array of good practice. They have created a series of short films
to help spread the word about coproduction, sharing good practice such as people with previous criminal convictions co-creating a website to inform employers on how they can empower and safely employ people who would normally be excluded from the jobs market.
The Scottish coproduction network seems to realise the importance of coproduction, with its annual Co-production Week, this year being held from 18th November
and focusing on ‘bringing people together from across the country to share ideas, learning and stories about how co-production puts people and communities at the heart of the support and services they’re a part of’ . Their online suite of resources
shows examples of coproduction with older people developing preventative care models
and coproducing dementia
services.
Coproduction in Wales
In August 2019, the Scottish coproduction network highlighted
the publication of Co-production Network for Wales’ new graphic which compares traditional approaches to public services to the co-productive approach. The background of the thinking behind this is described by Noreen Blanluet
in her blog post.
-
![]()
Click to enlarge
Button

Other more local and lesser known coproduction networks include:
- Side by Side Network – a London based coproduction network based in London, specifically Service User Network & Experience Bank for Coproduction supporting people involvement, innovation in mental health and peer support.
- Coproduction Norfolk – is a Peer Consultant & Change Agent, Pioneering In Mental Health & Social Care, aiming for a Social Movement For Equal Health
- Researchers or ‘think tanks’ like
UCL Centre for Co-production in Health Research are developing a collection of information to explore what co-creation is, what coproduction means in
everyday life and the honest difficulties of grappling with the word ‘coproduction’.
This are just a few examples of some of the coproduction work being done by organisations. We hope to share more and create a free and accessible coproduction database, so please feel free to share with us some of the work you are doing which you feel would come under the coproduction banner.
Our next blog will showcase a ‘coproduction reading list’ for those interested in the literature behind and backing up the coproduction idea and agenda.
Join us
We will be relying on a small but dedicated team and volunteers.
So, if you would like to be involved, please get in touch at hi@coproducecare.com
and help us open up the care debate, properly democratise care and please do join and share Coproduce Care:
Spread the word and uncover the hidden opportunities for people-led coproduced care
Recent Posts

We are pleased to provide an update our involvement in new projects currently being undertaken by Coproduce Care (CIC) in collaboration with Care and Support West. We will be contributing to local initiatives in Social Care Workforce Redesign, and we are excited to share the project with you. This project is running from June 2023 to June 2024. We will be working on three areas for the next 10 months all in the BNSSG region which are as follows: 1: Investigation of the Trusted Assessor Approach in Health and Social Care Systems In this project, we are investigating the Trusted Assessor Approach in health and social care systems. The objective is to demonstrate the value of Trusted Assessors in streamlining care needs assessment, while also addressing data protection and consent concerns. Case studies will be created from local regions that have implemented this approach, to provide insights into the benefits of Trusted Assessors of reducing delays in accessing required care. 2: BNSSG Opportunities for Levy Sharing and Increasing Apprenticeships in Social Care This project aims to identify opportunities for levy sharing in social care and increase the use of apprenticeships. The project will engage social care providers, training organizations, authorities, and other stakeholders to develop strategies, guidelines, and an implementation plan for utilizing the levy effectively and increasing the use of apprenticeships. 3: Integrated Health and Social Care: Enhancing Collaboration, Improving Quality, Shaping Models of Care, and the Future Social Care Workforce In this project, we are evidencing the enhanced collaboration between social care providers, health services, and local authorities. By mapping existing interfaces and collaborations, we seek to identify opportunities for cross-system benefits and improved outcomes, creating recommendations for integration for BNSSG. Our research will provide valuable insights to integration and collaboration between social care and health. At Coproduce Care (CIC), we believe that collaboration and innovation are vital for transforming social care. Through these projects, we aim to contribute to a more efficient and compassionate system. We extend our gratitude to all stakeholders, providers, commissioners, and policymakers for their invaluable support. Thank you for your continued interest in our endeavours. We will keep you updated as the projects progresses! In the meantime, if you are doing any work in any of these key areas, please get in touch with us using the below form. Thank you!

Dear Thérèse Coffey, We wish you the best of luck on your appointment as Secretary of State for Health and Social Care. Coproduce Care (CIC) is a non-profit organisation set up to democratise the social care debate. We support the voices of those working and involved in social care to influence wider decision making in the sector. Through our continued work in this area, we are writing to address some of the urgent needs of our social care workforce. We welcome your plans to set out ‘ Our plans for patients ’ to ensure our population have easier access to NHS and social care services through winter, putting the needs of patients as priority. To ensure we prioritise the health and wellbeing of our populations, and deliver the best, high-quality care possible, we need to ensure we prioritise the needs of our workforce who are at the front of delivering health and social care . To ensure both the health and wellbeing of our population and our social care workforce, we recommend the following: 1. Improving pay for social care workers, in real terms The Kings Fund published a report which compared the pay of social care workers to ten of the largest supermarkets. It found that nine out of ten supermarkets paid more than most social care roles. An example used is that if care worker left their role for a supermarket position at Tesco, they would see a 6.3% pay increase instantly. We have conducted many surveys, webinars, and connected with our audience on what is crucial to improving care workers working conditions and we have found that increasing pay is consistently the most crucial factor in reflecting the value of the work and high stress and responsibilities of the role . With the current cost of living crisis, this need for increasing pay is only getting more urgent. The sector currently has 100,000 vacancies , with extremely high levels of staff shortages. This affects the capacity to deliver services and the quality of care provided . Providers are struggling to recruit staff as they are competing with supermarkets and hospitality, sectors of which offer less stress and responsibility and more pay. We believe care workers are an invaluable part of our society and therefore should be paid accordingly. We recommend: · Introduce national pay scales that ensure care workers meet a real national living wage as a minimum . This will recognise the full contribution of social care workers make to the health of our population, and that their contribution is a real investment into our population. By increasing pay, we further increase recruitment and retention in the sector, and improve the perception of social care being a highly valuable and promising career choice. · Facilitate efforts to develop appropriate distribution of funds. Ensuring the integration and professionalisation of care is fully realised will allow better distribution of funds resulting in higher wages which better reflects the level of skill, qualifications, responsibilities and selflessness required to work within this sector. 2. Professionalising the care system Health and social care should be professionalised to encourage staff retention, career progression and further skill development. Professionalising care work would ensure that those working in the sector are valued and are provided with the necessary tools to provide high quality care. Currently, there is no accredited qualification for social care workers, without a standardised training process. We hosted a live stream with Gillian Keegan , who mentioned the government’s intention to create a voluntary digital care workforce hub, as well as a skill passport for all Health & Social Care workers. This is understood to allow easier identification of the workforce, including the possibility to share resources and opportunities to encourage the workforce to up-skill and develop. The skills passport would help keep track of the skills care workers have demonstrated over time, meaning career progression would be easier to identify . Whilst individual action is very important, to improve the quality of care, we urge for a standardised career and training development program for all care staff that results in an accredited qualification . We recommend: · Adequate pay to restore and recognise social care work as a valued profession . Extensive skills are involved in care work, and if standardised training and qualifications are implemented, security of applicable income is appropriate to these expectations. By increasing pay, care work has higher professional footing as a recognised career and role. · Ensuring the integration of social care is fully realised . The high fragmentation of the care sector and its lack of integration with NHS services makes it challenging to implement standardised training . The governments white paper ‘ Health and social care integration: joining up care for people, places and population ’ seeks the ambition to join up social care services. We welcome this white paper and its integration policy to achieve higher quality of care and better health outcomes. This ambition requires effort and commitment to the integration at all levels, and we hope that as health secretary, fully putting this policy into practice and reaching its scope, goals, and purpose is your focus in your new role. · Implementing standardised training, improved learning outcomes for workers, including IT, literacy, and numeracy training are addressed with sensitivity and with the voices of the workers at heart . Implementing standardised training would ensure a level of professionalism across the sector, however, must go in line with the security of increased income and security of hours of work. We must protect the wellbeing of our workforce, of which is already experiencing burn-out and exhaustion from the high pressures the sector is facing. We cannot have higher expectations of our workers undertaking standardised training without adequate pay . We hope you agree with our recommendations and seek to ensure we continue to improve the working conditions for our social care workforce. We hope that within your post as the new Health and Social Care Secretary, you prioritise the voices of those most impacted by decision making regarding the sector. Thank you for taking the time to read this letter, CoProduce Care Written by: Gabriella Neal

We wanted to investigate the issues around recruiting male care workers...